
Takeshi Kawamura
Associate Professor
Hospital Pharmacy Laboratory
Faculty of Pharma-Science
Teikyo University
This article introduces cases in Japan. (The SI NEWS Editorial Office)
Time is critically important in clinical settings. To facilitate team medicine, medical institutions have systems in place that not only allow different healthcare professionals to make accurate judgments and share information based on their expertise, but also to cooperate to accomplish things quickly. Many tests and analyses involving samples take time. Pharmacists are expected to quickly provide feedback of measurement and analysis results to physicians to help them understand and treat patients' conditions. In pharmacotherapy, blood drug concentration measurements provide critical information about the efficacy and risk of adverse reactions of a drug and guide patients to appropriate drug therapy. Speed is of the essence, since promptly reported blood drug concentration measurements can provide patients with the best drug therapy, whereas measurements reported late can be meaningless.
Accuracy is also critical, since measurements are associated with information about how long after dosing the sample was collected and are used by physicians to select future doses or pharmacists to make recommendations to physicians. The Pharmacy at Teikyo University Hospital is convinced that promptly and accurately determining blood drug concentrations for use in appropriate treatment design is the best way to help bring about optimal pharmacotherapy for patients. That is why we purchased the LM1010 high-performance liquid chromatograph. This article discusses our efforts to get this analytical instrument up and running in the hospital.
The story begins with a physician here asking if we could quickly provide blood concentration measurements of voriconazole. Until then, the hospital outsourced analysis to an external laboratory. A study found that patients suffer liver injury from voriconazole overdoses mainly 1 to 2 weeks after the start of treatment1). The external laboratory we used, however, took 4 days to 1 week after sampling to return the results, which were not very useful by the time they arrived. Consequently, few physicians placed orders. To address this issue, the hospital considered purchasing the LM1010 HPLC system, a certified medical device, for the pharmacy to use to determine blood voriconazole concentrations.
The list of drugs the LM1010 HPLC system could measure included mycophenolate mofetil, which a pharmacist had proposed analyzing for adverse reaction monitoring. The hospital has not used mycophenolate mofetil in organ transplant patients and is therefore not eligible to receive reimbursement for special pharmacotherapy management fees, but does often use the drug off label.
Pharmacists in the critical care ward use gas chromatography/mass spectrometry (GC/MS) in the pharmacy to perform drug toxicity analyses with patient plasma samples, but they needed a high-performance liquid chromatography (HPLC) system to accurately measure caffeine concentrations. GC-MS can screen samples for many drugs in one run and is therefore an important clinical tool for determining which drugs patients with consciousness disorders have used. However, GC-MS data are semi-quantitative, making them unsuitable for situations requiring accurate blood caffeine concentration data for patients with caffeine poisoning.
The pharmacy therefore purchased the LM1010 HPLC system (Hitachi High-Tech Science Corporation) to allow it to promptly provide blood concentrations of voriconazole, mycophenolate mofetil, and caffeine to healthcare professionals for use in caring for their patients. The ability of the LM1010 to precisely measure voriconazole and mycophenolate mofetil concentrations makes it suitable for use in clinical settings2,3). We created an area for the LM1010, appointed analysts, and evaluated the stability of the measurements conducted by the analysts in preparation for operating the instrument in the hospital.
We began by establishing a working group for blood drug concentration analyses in the pharmacy. The group consisted of pharmacy personnel in charge of GC-MS, pharmacists in the infection control unit, and the assistant manager in charge of pharmacy operations and research. To get everyone on the same page, the group discussed the information related in “Clinicians Ask for Help” above and shared the goals for procuring an HPLC system.
Hitachi High-Tech Science Corporation recently developed a medical device authorized for clinical use based on the principles of HPLC, the LM1010. The LM1010 HPLC system has a listed marketing notification number as a general medical device (i.e., a specially-designated medical device requiring maintenance). It automatically verifies performance and can be used by even unskilled operators to determine concentrations in a stable manner. The clinical usefulness of the accurate measurements promptly provided by the LM1010 has been discussed in papers and conference presentations.
Although the pharmacy does not appoint a pharmacist dedicated to the LM1010 because hospital physicians do not place orders every day, it must be ready to quickly process orders. A pharmacist assigned to the hospital’s critical care ward is on call on weekdays to analyze samples with GC-MS when orders are placed. Although this pharmacist is trained on liquid chromatography and would ideally perform drug concentration analyses with LC, this pharmacist may not be able to perform analysis with the LM1010 in addition to GC-MS in emergencies. The pharmacy therefore called on pharmacists assigned to other wards to build a team of four analysts charged with operating the instrument.
To ensure infection control, we created an area for the LM1010 and installed it in the pharmacy in preparation for its eventual use. Column operation and other pretreatment with patient serum or plasma are done in the critical care ward. Pretreated samples are then brought to the pharmacy to be analyzed in the LM1010. We installed a refrigerator in the pharmacy laboratory to store samples for potential re-analysis when the results of the initial analysis are abnormal or inappropriate. We also sought understanding about where and how to analyze temporarily stored serum and plasma samples, as well as related safety issues, through pharmacy manager meetings and pharmacy personnel meetings.
A team of multiple analyst is needed to promptly process orders, and each analyst must be capable of correctly and accurately analyzing samples to ensure consistent results. To prepare the analysts, we trained them and then assigned two tests for each drug. The results are presented in Table 1. The first test involved determining the drugs at known concentrations (reproducibility test). For mycophenolate mofetil and caffeine, we had the analysts analyze filtered serum samples spiked with known concentrations of these drugs (serum spike recovery test). Analysts were tested to see if they were able to properly determine the concentrations.
The analysts analyzed samples containing 2.5 μg/mL voriconazole, 5.0 μg/mL mycophenolate mofetil, or 50 μg/mL caffeine.Values within 20% of the true value were deemed acceptable. Analyst operability was assessed as acceptable when all measurements were within 20% of the true value.
The HPLC (LM1010) measurements by the analysts were 2.6±0.1 μg/mL for the 2.5 μg/mL voriconazole sample, 4.4±0.2 μg/mL for the 5.0 μg/mL mycophenolate mofetil sample, and 51.1±5.3 μg/mL for the 50 μg/mL caffeine sample. The percent differences between the prepared concentrations and measured concentrations (mean absolute percent error) were 5.4%, 11%, and 4.4%, respectively. All values differed from the true value by no more than ±10%, ±15%, and ±15%, respectively.
Table 1 Reproducibility test and serum spike recovery test (n=3)

Mycophenolate mofetil requires therapeutic dose monitoring because its bioavailability differs widely among individuals, and because drug interactions have been reported in association with calcineurin inhibitors, which may be used in combination with the drug. Since no orders for mycophenolate mofetil analysis had ever been placed with the Central Laboratory, we prepared a sample by spiking standard human serum with mycophenolate mofetil for use in the serum spike recovery test.
The concentration determined using HPLC (LM1010) for the serum sample spiked with 5.0 μg/mL mycophenolate mofetil in the serum spike recovery test was 4.5±0.6 μg/mL. The average percent difference between the prepared concentrations and measured concentrations (mean absolute percent error) was 12%. All values differed from the concentration of 5.0 μg/mL by no more than ±20% (Table 1).
Serum samples spiked with caffeine at concentrations of 50 and 25 μg/mL were analyzed using HPLC (LM1010) in a serum spike recovery test; the measured concentrations were 49.8±0.4 and 24.3±1.4 μg/mL, respectively. The average percent differences between the prepared concentrations and measured concentrations (mean absolute percent error) were 0.8% and 4.6%, respectively. All values differed from the concentration of 50 μg/mL by no more than ±5% and ±10%, respectively (Tables 1 and 2).
We must be able to accommodate orders for voriconazole and mycophenolate mofetil analysis from all hospital departments. We made a “Request analysis” button on electronic medical record forms and asked the Central Laboratory to help perform analyses with sample tubes collected in the Central Laboratory, as for other blood tests. In collaboration with the Administration Department, we stopped outsourcing voriconazole analysis and began doing it in the pharmacy.
The pharmacy accepts orders from 9:00 a.m. to 3:00 p.m. on weekdays (Monday to Friday) and generally returns results on the day of the order. The final deadline, however, is 5:00 p.m. The result deadline is set for three hospital days after the order (with the day of the order included) to allow for when pharmacy analysts are away or analysis is not possible because the pharmacy is handling an emergency. Reports are sent to the Central Laboratory when it has personnel available for accepting reports, i.e., 8:30 a.m. to 5:00 p.m. on weekdays and 8:30 a.m. to 12:30 p.m. on Saturdays.
We had to choose between plasma and serum samples and, for voriconazole, chose serum samples to maintain existing processes, since serum was the type of sample used by the contract laboratory. For mycophenolate mofetil, we chose EDTA-treated plasma samples, which were the type of samples used by the contract laboratory. To determine whether the drugs could be measured in plasma, we purchased standard human plasma, spiked it with mycophenolate mofetil and caffeine, and performed a plasma spike recovery test. Standard human plasma did not pass through a filter with a pore size of 0.45 μm (filter diameter: 13 mm). Plasma did, however, pass through a hydrophilic PTFE filter with a pore size of 0.45 μm (filter diameter: 33 mm, effective filtration area: 5.1 cm2). Measured concentrations were ±15% of the true values. We repeated this process for caffeine (Table 2). Ultimately, we decided to measure mycophenolate mofetil and caffeine concentrations in plasma samples processed using a filter with a pore size of 0.45 μm (filter diameter: 33 mm).
Table 2 Comparison of spiked concentrations to measured concentrations in plasma and serum (n=3)

Our proposal involved changing current hospital testing operations and therefore had to be reviewed by the Clinical Laboratory Board. The pharmacy drafted a request letter that proposed the procedures and a workflow for blood drug concentration analysis. To allow us to meet the needs of clinicians to obtain results promptly, we asked the hospital to allow the pharmacy to measure voriconazole and mycophenolate mofetil concentrations and report the results, and we also asked that voriconazole analyses stop being outsourced. Our request letter presented a description of the request, procedures, blood sample types, and treatment, a description of the change to electronic medical record forms, hours of order acceptance, reporting deadlines, and requested start dates.
The Clinical Laboratory Board reviewed the proposal and granted approval for the pharmacy to perform blood drug concentration analysis, but they submitted an opinion that results should be shared throughout the hospital so that healthcare professionals can access the results when they need them. Including measurements as entries in electronic medical records would have been ideal, but presented a problem. The Central Laboratory is ISO 15189-certified and is required under the review requirements of this certification to directly input results into electronic medical records. The contract laboratory was also ISO-certified and therefore able to enter results, but the pharmacy was unable to enter the results it determined. Under a solution proposed by the Central Laboratory, we decided to create a new area to enter test results for voriconazole and other analyses performed by the pharmacy. In the margin of printed reports, we included the text “Results indicated as being from the pharmacy are non-ISO 15189.” This allowed the listing of results in the test results area and viewing of test values throughout the hospital.
We made buttons for ordering tests for voriconazole and mycophenolate mofetil between the “Managed by the pharmacy” and “Toxicity analysis by pharmacy” buttons at the lower right in the blood drug concentration tab under the sample tests/serum chemistry tests area in the electronic medical record form (Figure 1). We had to shorten the text on the mycophenolate mofetil button because we needed to indicate that the pharmacy would be doing the tests and because “mycophenolate mofetil” is too long to fit within the allotted button space. After deliberating whether to name the test by the drug name or analyte name, we decided to label the button “Pharmacy: Mycophenolate” to reduce the likelihood of errors.
The laboratory sent the following all-personnel email about the changes made to testing (Figure 1).
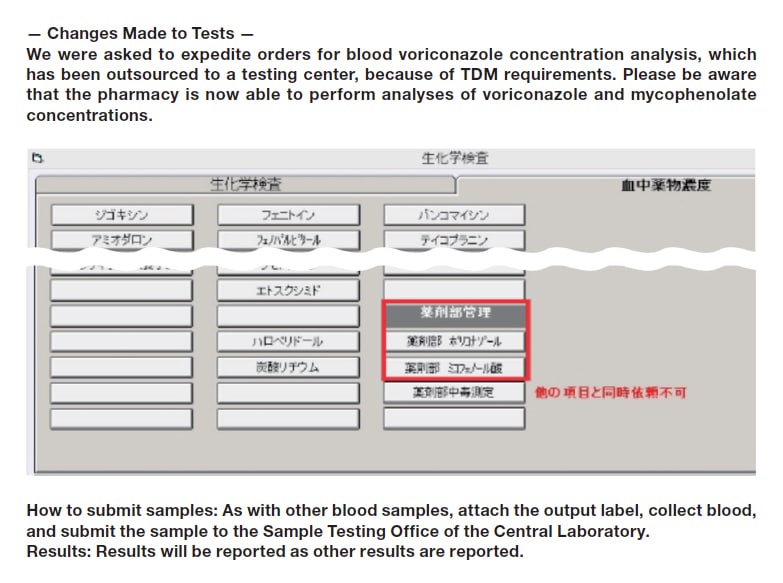
Fig. 1 Raising awareness in the hospital
Note: The image in the figure is a screen capture in Japanese.
The workflow spanning from ordering to the reporting of results is described here. First, a physician from any department places an order for blood drug concentration analysis in the electronic medical records. Blood is sampled at an appropriate time. The sampling tube is delivered to the Central Laboratory. The Central Laboratory centrifuges the tube and then notifies the pharmacist responsible for blood concentration analysis in the pharmacy that a plasma or serum sample is available. That pharmacist contacts the pharmacist in charge of analysis that day. The analyzing pharmacist receives a form for entering information about the sample and results from the Central Laboratory. (A label identical to the label attached to the sample is attached to the form.) The analyzing pharmacist then filters the sample, pretreats a spin column, and analyzes the sample with the LM1010 in the pharmacy. The pharmacist writes the measurement on the form and sends it to the Central Laboratory via the hospital’s pneumatic tube system. The Central Laboratory enters the result in the patient’s electronic medical record. A pharmacy analyst confirms that the result entered in the electronic medical record is correct and notifies the pharmacist in the ward in question depending on whether the blood concentration is in the appropriate range. Finally, the ward pharmacist shares the information with ward personnel to use to formulate a treatment plan.
Many hurdles faced the inclusion of blood drug concentration analysis for the hospital in the list of duties performed by the pharmacy. Cooperation throughout the institution, however, made this possible at Teikyo University Hospital, which prides itself on a team care approach. I am convinced that we were able to begin offering analyses thanks to the cooperative nature of the hospital’s personnel and their desire to contribute to patient welfare. Even now, the pharmacy continues to analyze samples and report the results without a hitch. Since physicians learn the results on the day of analysis, orders particularly for voriconazole analysis have grown substantially. Collaboration will be increasingly important for new projects in the future. To allow this to happen, we are committed to building trust among healthcare professionals.
Acknowledgments
The commissioning of the LM1010 in the pharmacy was made possible with the assistance of Taiji Furukawa, Director, department of central laboratory, Teikyo University Hospital, as well as Chief Technician Yukiko Okufuji, Pharmacy Director Nobuhiro Yasuno, Pharmacy Assistant Director Yoshiharu Mitsunaga, and many others. Pharmacy analysts Shoichi Imanaka, Tatsuro Kuwahara, and Mensah Joshua also greatly assisted in the project. Finally, employees of Hitachi High-Tech Science were kind enough to provide information about the LM1010. I am grateful for everyone’s kind contributions.
References
See more
