
Hideki Hashimoto
MD & PhD
Manager of the Department of Emergency and Critical Care Medicine and Chief of Emergency and Critical Care Center,
Hitachi General Hospital
Associate Professor,
Department of Infectious Diseases,
Hitachi Medical Education and Research Center,
University of Tsukuba Hospital
Sepsis is defined as “a condition in which a dysregulated host response to an infection leads to serious organ dysfunction1).” Sepsis represents the most severe form of infection, with 20% to 30% of cases being fatal. Relevant Japanese and international guidelines stress appropriate early intervention as the key to improving outcomes, and one intervention is the early administration of appropriate antibiotics1,2).
Conventional approaches for selecting appropriate antibiotics have focused on rapidly administering an antibiotic effective against the causative microorganism. More recent approaches, however, also emphasize optimizing the dose regimen by determining how much drug should be administered and at what dosing interval. Studies are producing a growing body of evidence about the continuous infusion and extended infusion of beta-lactam antibiotics frequently used in sepsis management, as well as therapeutic drug monitoring (TDM). This article presents the theoretical underpinnings of and current evidence supporting these approaches and also discusses the use of rapid bedside TDM in ICUs, which has recently become more prevalent.
Patients with sepsis often have blood antibiotic concentrations outside the appropriate window because of substantial changes in pharmacokinetics caused by the following physiological alterations3).
(1) Increased volume of distribution: Sepsis causes increased vascular permeability, leading to extravasation of fluids. High-volume fluid resuscitation also increases effective circulating volume. These changes greatly increase the volume of distribution of water-soluble antibiotics, lowering their concentrations in the blood. Many critically ill patients have hypoalbuminemia. In those with hypoalbuminemia, highly protein-bound antibiotics occur less as protein bound and more in the unbound form. More drug moves to the tissues, increasing the volume of distribution as a result.
(2) Augmented renal clearance: Sepsis-associated inflammation, high-volume fluids, and catecholamine administration can increase renal blood flow, pushing renal function beyond normal levels. This condition is known as augmented renal clearance (ARC) and is typically defined by a 24-hour creatinine clearance (CrCl) of greater than 130 mL/min/1.73 m2. Young males and those with trauma/head trauma, burns, or sepsis are at increased risk of ARC. In a meta-analysis of critically ill adults, ARC was seen in 39% of the overall population and 33% of those with sepsis4). Those with ARC experience the early elimination of renally excreted drugs and have difficulty achieving target concentrations at standard doses.
(3) Decreased clearance from organ dysfunction: Sepsis frequently causes acute kidney injury, and this results in a condition opposite to ARC. Delayed drug elimination due to decreased renal function leads to overdosage at standard doses, which in turn increases the risk of adverse events due to elevated blood concentrations (e.g., neurological, hepatic, and renal adverse events due to beta-lactam antibiotics). Patients with this condition are often on extracorporeal membrane oxygenation (ECMO) or continuous hemodiafiltration (CHDF). The changes these cause in drug absorption and removal and volume of distribution reduce blood concentrations. Blood concentrations become even more difficult to predict as a result.
The takeaway points are that there is substantial variation in pharmacokinetics among individual patients with sepsis, and that some patients have insufficient (or excessive) levels when treated at normal antibiotic doses.
Beta-lactam antibiotics are a class of agents characterized by time-dependent antimicrobial activity. Their efficacy is therefore highly dependent on the proportion of time during which their blood concentration exceeds the minimum inhibitory concentration (MIC) of the responsible microorganism (%T>MIC): the longer this time, the greater their antimicrobial activity. A %T>MIC of 40% to 70% is a typical target i n general infection management. Given that critically ill patients require higher concentrations, the European Society of Intensive Care Medicine recommends a %T>MIC of 100% in a position paper5). One guideline recommends continuously exceeding the level at 4 times MIC (100% fT>4×MIC) 6).
In practice, however, these targets are often not achieved. In an international multicenter study of beta-lactam antibiotic blood concentrations in patients in the intensive care unit (ICU) for sepsis and other conditions, the target 100%fT>MIC was not achieved in almost 40% of the patients7). Insufficient antibiotic levels should be avoided because they lead to treatment failure and the development of resistant strains. Sufficient antibiotic levels must therefore be maintained in critically ill patients in particular.
Continuous infusion and extended infusion are two approaches based on the pharmacokinetic/pharmacodynamic (PK/PD) characteristics of beta-lactam antibiotics for achieving target levels. For example, infusing meropenem or piperacillin/tazobactam continuously or as an extended infusion (of at least 3 hours) produces concentrations above MIC with fewer troughs than when these drugs are given as intermittent infusions of 30 minutes to 1 hour (Figure 1). Continuous infusion keeps concentrations above MIC throughout the day, which is particularly beneficial for patients with ARC or otherwise augmented renal clearance, critically ill patients, and patients infected with a microorganism with a high MIC. Continuous and extended infusions are now widely used in American and European ICUs. In an international, multicenter survey whose results were published in 2023, beta-lactam antibiotics, when used, were given as an extended or continuous infusion in about 60% of ICUs8).
Evidence supporting the continuous infusion of beta-lactam antibiotics is growing. Suffering from small sample sizes, the studies conducted through 2023 failed to sufficiently demonstrate efficacy. However, in 2024, the results of an international, multicenter, randomized, controlled trial (RCT) showing the benefit of continuous meropenem and piperacillin/tazobactam infusions in 7200 patients with sepsis (the BLING III trial) were announced9). No significant difference in mortality at day 28 was shown between the patients given continuous and intermittent infusions, whereas the former population achieved better improvement in clinical symptoms. A 2024 meta-analysis of 18 RCTs including BLING III (total of 9108 patients) found significantly lower mortality at day 90 associated with continuous/extended infusion (25.7% for extended vs. 28.2% for intermittent, relative risk: 0.86, 95% CI 0.72-0.98), as well as improved clinical cure rates10). Such evidence has demonstrated the benefit of continuous infusion of beta-lactam antibiotics for sepsis to an extent to which this therapy is weakly recommended in Japanese and international guidelines on sepsis management1,2).
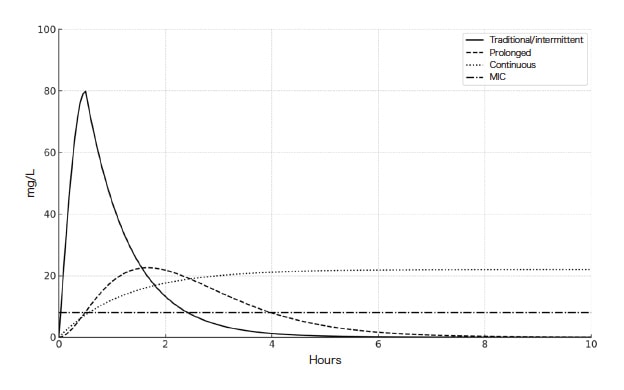
Fig. 1 Changes in blood concentrations of beta-lactam antibiotics given with different infusion approaches
Maintaining sufficient blood levels of antibiotics in patients with sepsis is key to treatment success, even though adequate levels are often not achieved in practice. Developing treatment strategies such as continuous infusions may improve exposure, but whether a patient has achieved an appropriate blood concentration is still unclear. Betalactam antibiotics are generally well tolerated, but they can be hazardous at extremely elevated blood concentrations. One study found that the risk of neurotoxicity increased to 50% at trough concentrations exceeding 360 μg/mL of piperacillin and 64 μg/mL of meropenem11). Though the adverse events reported in the continuous infusion arm of the BLING III trial did not differ significantly from those in the intermittent infusion arm, serious central neurological adverse events were reported in the continuous infusion arm, and elevated blood concentrations may have been involved. Blood concentrations must be appropriately managed to both ensure therapeutic efficacy and avoid adverse events. For this, TDM is a solution for measuring blood concentrations and adjusting doses.
In TDM, the blood concentration of a drug is measured, with the results used to adjust the dose or dosing interval. TDM is performed to optimize the efficacy and safety of pharmacotherapy in patients and is used mainly with drugs having a narrow therapeutic window or large inter-individual variation in pharmacokinetics. Beta-lactam antibiotics were not the subject of routine TDM given their relatively wide safety margin, but more experts are calling for TDM for beta-lactam antibiotics to be used in the management of severe infections.
Data suggest that using TDM may improve clinical outcomes in severe infections. In a multicenter RCT, Hagel et al. compared TDM with conventional practice in 249 patients with sepsis treated with continuous infusions of beta-lactam antibiotics (piperacillin/tazobactam). Significantly more of those managed with TDM achieved target concentrations than those managed without TDM (37.3% vs. 14.6%)12). A meta-analysis of 8 studies that included this trial concluded that TDM might reduce treatment failure, although the heterogeneity of the studies was high13). The Japanese Clinical Practice Guidelines for Management of Sepsis and Septic Shock 2024 weakly recommends (Grade 2D) “Administering antibiotic treatment with TDM in sepsis.”1) These developments show the increasingly prominent role of TDM in sepsis management. More institutions are adding TDM to their treatment protocols. The above-mentioned, international, multicenter study found that about 40% of responding institutions used TDM for beta-lactam antibiotics, and that the proportion exceeded 50% in institutions in Europe and Central and South America8). As these highlights of the above studies suggest, TDM for beta-lactam antibiotics is attracting attention as an effective tool for better managing sepsis and preventing antimicrobial resistance.
A growing body of evidence supports TDM for the anti-MRSA drug linezolid in addition to beta-lactam antibiotics. Linezolid is commonly used to treat severe infections such as ventilator-associated infections, but it can cause myelosuppression (e.g., thrombocytopenia, anemia) as an adverse reaction. The likelihood of linezolid causing myelosuppression grows with both prolonged administration and elevated blood concentrations. A study found that blood trough concentrations exceeding 7 μg/mL increase the incidence of thrombocytopenia and proposed a target blood concentration of 2 to 7 μg/mL to achieve therapeutic efficacy while avoiding adverse events7). Since linezolid is typically given at a predefined dose regimen irrespective of renal function, overdoses can occur in patients with certain background factors. Advanced age and renal failure are known to increase the likelihood of elevated blood concentrations. In a study involving patients aged 65 years or older, over half of the patients had trough concentrations exceeding the target range14). In my practice, I have encountered patients with sepsis on blood purification therapy due to renal failure who have quite high blood concentrations after linezolid administration and suffer myelosuppression in the early stages of treatment.
The findings of a meta-analysis suggest that TDM could prevent serious adverse reactions15). There have been recent attempts to use TDM for linezolid to adjust the dosage to individual patients and thereby reduce the risk of adverse reactions.
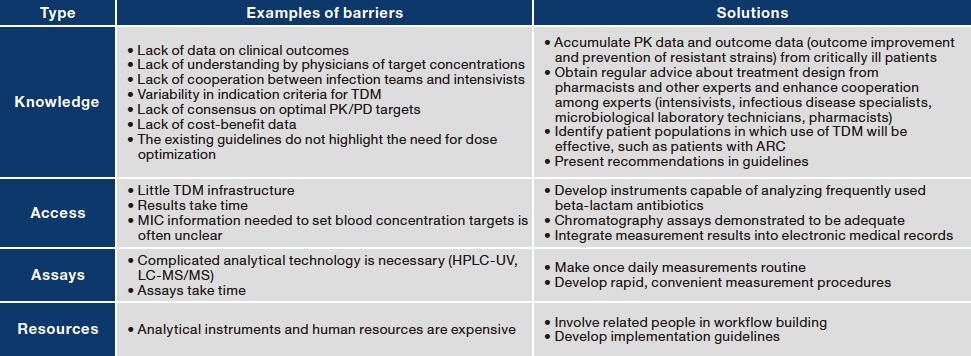
As mentioned above, despite its theoretical benefits, TDM for beta-lactam antibiotics and linezolid has yet to be widely adopted in Japan. Several hurdles are responsible (Table 1). The largest of them are a lack of evidence involving hard outcomes such as mortality and the previous absence of instruments that allowed convenient measurements.
Table 1 Major barriers impeding the adoption of TDM for beta-lactam antibiotics (created by the author in reference to Reference 16)
The apparent benefits of TDM in theory contrasts with the lack of evidence in clinical practice. The study of Hagel et al. cited earlier found that the TDM arm achieved target blood concentrations significantly more than the control arm, but there was no significant difference in 28-day mortality (21.6% vs. 25.8%)12). A meta-analysis that included the study of Hagel et al. and three other RCTs together with seven observational studies concluded that TDM reduced clinical symptoms and improved biological cure rates, but it did not significantly lower mortality17). In a subsequent Dutch, multicenter RCT in patients admitted to the intensive care unit (DOLPHIN trial), neither mortality nor ICU length of stay differed between patients treated with TDM and those treated with standard dosing18).
There are several potential reasons for the lack of valid evidence involving hard outcomes such as mortality. First, previous studies were not limited to populations that would most likely benefit from TDM. Moreover, it takes time to initiate TDM after antibiotic treatment has begun. Finally, no studies with sufficient statistical power have been conducted. The RCT of Hagel et al., for example, had a high target blood concentration (4 times MIC), yet it targeted mostly susceptible causative microorganisms. The patients may therefore have achieved 100% fT>MIC even without TDM. The sample size of this RCT allowed the detection of a difference in the primary endpoint (SOFA score, or severity score), but the statistical power was likely insufficient to evaluate mortality. Of the diverse array of drugs used in the DOLPHIN trial, the most common was ceftriaxone, which has a long half-life. Moreover, the median time from the start of treatment to initial intervention was long (20 hours). As a result, target concentration achievement was comparable between the TDM and standard dosing arms. Reflecting on these studies, I am convinced that it would be more efficient to limit the use of TDM for beta-lactam antibiotics to specific populations that would most likely respond to continuous infusions, rather than to all patients with sepsis. Specific examples of populations for whom TDM should theoretically be indicated include: (1) critically ill patients with ARC or on CHDF or ECMO, who exhibit substantial variability in pharmacokinetics; (2) patients with burns or obesity; (3) patients infected with a high-MIC pathogen; and (4) patients on drugs such as meropenem or piperacillin/tazobactam that have a short half-life and are frequently used in sepsis management19). More evidence, however, is needed to verify these indications.
Another major barrier to implementing TDM is the need for proper equipment and technical expertise in general. Conventionally, measuring blood concentrations of beta-lactam antibiotics has required chromatography and been a complex, time-consuming process. The recently developed LM1010 high-performance liquid chromatograph may offer a solution. The LM1010 is a sophisticated analytical instrument that is designed to be easy to operate. Users can operate the instrument with no special technical expertise. With the LM1010, blood concentrations of meropenem, piperacillin, linezolid, and other antibiotics frequently used in intensive care settings can be quickly determined in-house. Using this instrument could break down many of the existing barriers and help generate evidence. We have an LM1010 in the ICU of our hospital that ICU-based pharmacists and intensivists use to determine blood concentrations in real time (Figure 2).
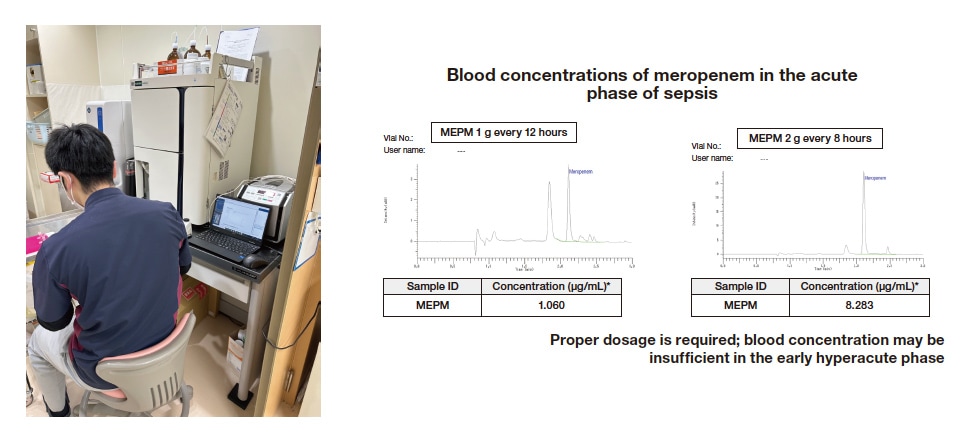
Fig. 2 Using the LM1010 for blood concentration analysis
Providing proper antibiotic therapy is key to improving the outcomes of patients with sepsis, and TDM is an important tool for achieving this goal. Recently developed analytical instruments and accumulation of knowledge are making quick implementation of TDM for drugs such as beta-lactam antibiotics and linezolid possible at the bedside. Although cost-related and other issues remain for implementation, the wider use of TDM promises to further improve the quality of sepsis management and lead to better outcomes for patients.
References
See more
