
Kazuaki Matsumoto
PhD
Professor
Division of Pharmacodynamics,
Keio University Faculty of Pharmacy
Microorganisms are responsible for all human infections. Figure 1 shows the relationships between people, causative pathogenic microorganisms, and antimicrobial agents. The causative organisms cause infections in humans, and antimicrobial agents exhibit antimicrobial activity against the causative organisms. In addition to the immunologic response to the microorganisms, humans are also involved in the processes of absorption, distribution, metabolism, and excretion of antimicrobial agents. On the other hand, antimicrobial agents can cause adverse reactions in humans and may induce bacterial resistance. Therefore, appropriately used antimicrobial agents are therapeutic agents for infectious diseases, but their inappropriate use induces side effects in humans and resistance in bacteria. Therefore, antimicrobial agents must be used appropriately.
Antimicrobial stewardship (AS) comprises a team of physicians, pharmacists, laboratory technicians, and nurses specializing in infectious diseases, aims to support the attending physician in using antimicrobial agents to maximize the therapeutic effect on individual patients, minimize adverse events as much as possible, and complete (optimize) the treatment of infectious diseases as quickly as possible. Since careless (inappropriate) use of antimicrobial agents causes the development or spread of resistant bacteria, promotion of AS can prevent or delay the emergence of resistant bacteria and reduce medical costs, according to the Guidance for the Implementation of Antimicrobial Agents Guidance for implementation of programs to support appropriate use of antimicrobial agents1).
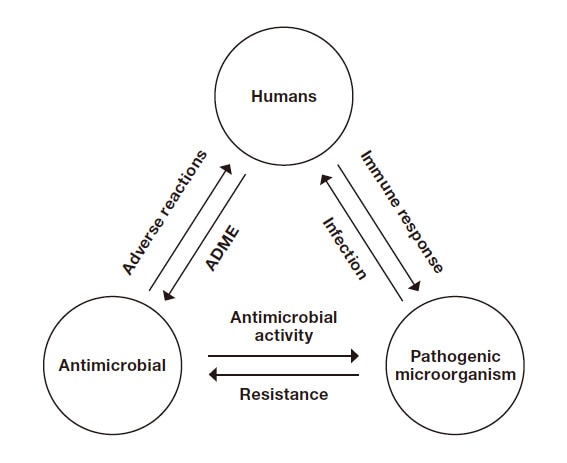
Fig. 1 Relationships between humans, causative pathogenic microorganisms, and antimicrobial agents
ADME: Absorption, distribution, metabolism, and excretion
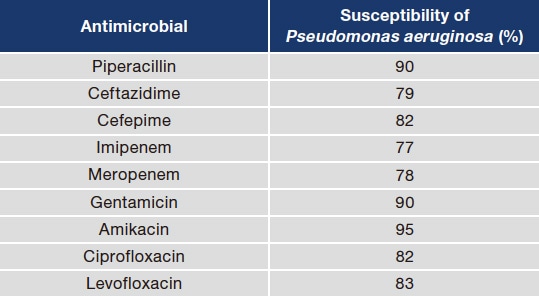
Before deciding on an antimicrobial regimen for treating a suspected infection, clinicians must (1) first determine whether an infection is present. Diagnosis of infections cannot be confirmed based on fever alone. Conditions such as drug-induced fever, collagen disorders, malignant lymphoma, thromboembolism, and dehydration, etc., must be carefully ruled out. If an infection is confirmed, (2) the next step is to identify which organs are affected. Since different pathogenic microorganisms infect organs at different rates, identifying the affected organ will help (3) predict the causative microorganism. Knowing the age and underlying diseases of the patient and where the infection originated, such as in the community or in a hospital, will further narrow down the list of suspected microorganisms. Once the causative microorganisms are identified, (4) antimicrobial agents to which the microorganisms are susceptible should be selected. From the antimicrobial spectrum of various antimicrobial agents, select an antimicrobial agent that has antimicrobial activity against the assumed bacteria, and is highly susceptible according to the antibiogram, taking into account of the patient background, the breadth of the antimicrobial spectrum, and interactions. As an example, an antibiogram showing susceptibility of Pseudomonas aeruginosa in a medical institution is shown in Table 1. Since the low susceptibility to carbapenem drugs in this institution suggests a likelihood of treatment failure, a non-carbapenem antimicrobial should be selected if Pseudomonas aeruginosa were suspected.
Table 1 Sample antibiogram
Antimicrobial treatment is termed different according to when it is initiated over the course of the infection (Figure 2). Prophylactic therapy is used to prevent infections that may occur in the future, although the patient has not yet developed an infection. (Preoperative treatment is a typical example). Once an infection is established, the antimicrobial agent to use is selected by predicting the causative pathogenic microorganism according to steps 1 to 4 mentioned above. Antibacterial treatment given when the pathogenic microorganism is unknown and susceptibility data are unavailable is called empiric therapy (pending for culture results). Antimicrobial therapy is administered after the causative microorganism is confirmed by the culture results, and susceptibility results are known is called optimal (targeted) therapy.
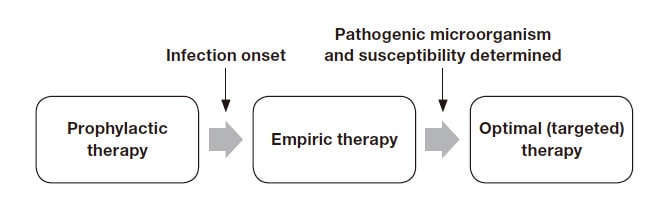
Fig. 2 Designations of antimicrobial therapy
Once a specimen has been collected, 3 days are required to determine the causative pathogenic microorganism and its susceptibility (Table 2). Empiric therapy is initiated against the suspected pathogenic microorganism. Gram staining, which takes about 15 minutes, is performed to further narrow down the causative microorganism. Figure 3 shows phagocytized gram-positive cocci that have been Gram-stained. Since the bacteria look like grapes, indicating that they are staphylococci. Knowing it is a staphylococcal bacterium, even though the species has not been identified and drug susceptibility data are pending, cefazolin or vancomycin can be recommended.
Table 2 Bacterial culture and antimicrobial therapy
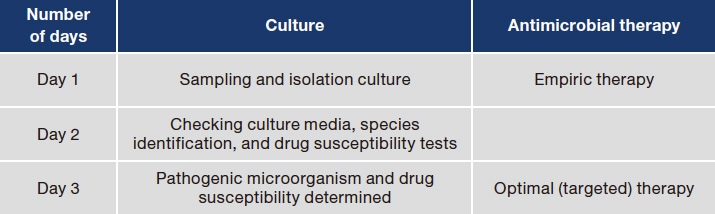
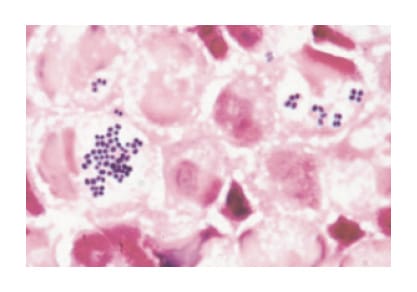
Fig. 3 Detection of gram-positive cocci with Gram staining
Source: Nagata K., Gram Staining Informs Infection
Diagnosis. p. 15, 2006 [in Japanese].
In severe infections such as septic shock, the survival rate of patients can be improved by administering antimicrobial agents that are sensitive to the causative organisms as early as possible2). Since cefazolin is effective against staphylococcal bacteria3), and vancomycin is effective in resistant staphylococcal bacteria, treatment with a combination of both drugs should be considered in severe cases. Thus, severe infections in which staphylococcal bacteria have been detected are empirically treated with a regimen of cefazolin and vancomycin. If the causative organism and drug susceptibility are identified on day 3, monotherapy with either antimicrobial agent should be used as optimal (targeted) therapy. As mentioned earlier, unnecessary antimicrobial agent use can cause adverse reactions and induce bacterial resistance, leading to detrimental financial consequences. Shortening the time needed for obtaining bacterial tests results therefore is essential to facilitate the acceleration of proper antimicrobial use.
Verigene®, an automated concurrent multi-parameter gene-based testing system, uses microarray technology to concurrently detect bacteria and drug-resistance genes within 3 hours after a positive blood culture result is obtained. The kit detects the drug-resistance genes mecA, vanA, and vanB in gram-positive bacteria and CTX-M, KPC, NDM, VIM, IMP, and OXA in gram-negative bacteria. Figure 4 illustrates a procedure for bacterial tests, selecting antimicrobial therapy, and optimizing therapy in severe infections. An example is a case in which vancomycin is used to treat an MRSA infection. Verigene® system identifies the pathogenic microorganism (Staphylococcus aureus) and its drug-resistance gene (mecA) the following day after gram-positive bacteria are detected in the blood sample. At this point, a decision can be made to discontinue cefazolin and continue vancomycin from the empiric therapy regimen of cefazolin and vancomycin. Had the pathogenic microorganism been Enterococcus faecium and the drug-resistance gene vanA been detected, both antibiotics would have been discontinued and switched to linezolid treatment. Verigene® system allows optimal (targeted) therapy to be initiated the next day after blood sampling contributes greatly to promoting AS.
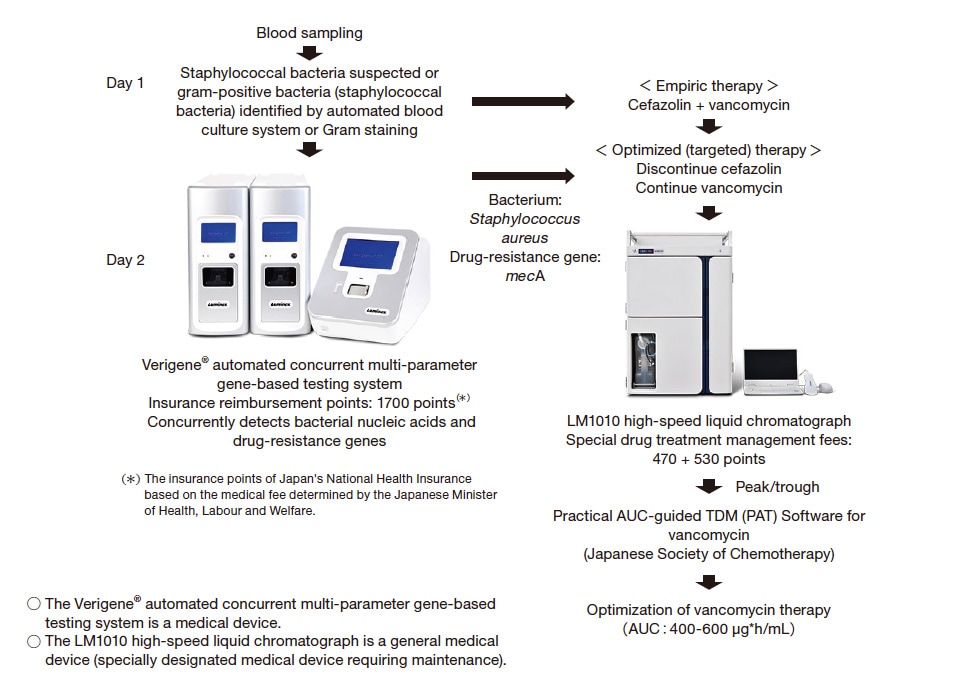
Fig. 4 Optimizing therapy in a patient with a severe infection based on bacterial testing and blood drug concentration measurements (example for MRSA treated with vancomycin)
Therapeutic drug monitoring (TDM) starts from the initial treatment dosage design, measuring blood concentrations of drug after the start of treatment, and revising the dosage to ensure that treatment is safe and effective. TDM is used for drugs with a narrow target blood concentration window, such as glycopeptide and aminoglycoside antibiotics, and the antifungal agent voriconazole. Antimicrobial agents are dosed based on their pharmacokinetic/pharmacodynamic (PK/PD) parameters correlated with efficacy and safety. In TDM, target drug blood concentration windows are selected based on PK/PD data.
PK/PD refers to associating and analyzing changes over time in blood concentrations (PK) and pharmacological effects (PD) in an individual by means of model analysis. For example, by clarifying the relationship between the occurrence of side effects (PD) and drug blood concentration (PK) from the aspect of safety through PK/PD analysis, an index of blood concentration avoiding side effects can be determined. On the other hand, from the perspective of efficacy in the field of infectious diseases, minimum inhibitory concentration (MIC) that reflects the drug sensitivity of the causative microorganism is a PD indicator that can be combined with different PK parameters such as the ratio of the area under the blood concentration-time curve (AUC) to MIC, the ratio of Cpeak to MIC, and time above MIC in infections, to be called PK/PD parameters. The mechanisms of action of different antimicrobial agents based on PK/PD parameters are shown in Table 3. Aminoglycosides, for example, have a concentration-dependent efficacy profile. Since their efficacy is dependent on Cpeak/MIC, administering a total daily dose once daily to obtain higher peak values is therefore recommended over administering multiple times a day. Beta-lactam drugs have a time-dependent efficacy profile. They remain effective when their concentrations are kept above the MIC. Accordingly, it is recommended that a total daily dose be given 3 or 4 times daily instead of 1 or 2 times a day. Vancomycin, linezolid, and voriconazole fall under the AUC/MIC classification. In a clinical study, Scaglione and colleagues compared a group of patients given antimicrobial therapy based on PK/PD data to a group treated without using PK/PD data. The former had shorter hospital stays, fewer non-responders, and fewer deaths. These findings show that administering antimicrobials based on PK/PD data improves treatment outcomes4). The present research findings recommend administering antimicrobial agents based on PK/PD data.
Table 3 PK/PD parameters considered for different antimicrobials
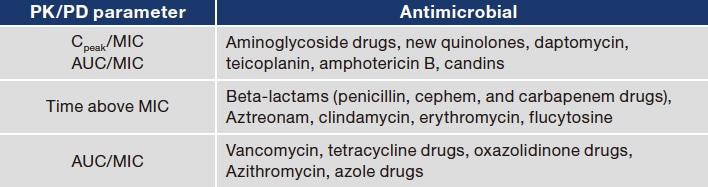
PK/PD: pharmacokinetics/pharmacodynamics, Cpeak : peak value, AUC: area under the blood concentration-time curve, MIC: minimum inhibitory concentration
Table 4 lists antimicrobial agents indicated for TDM, the days on which blood concentrations are determined with their associated target values. Among the TDM drugs, vancomycin is the one whose index will be changed after 2021. AUC is the PK/PD parameter most closely correlated with the efficacy and safety of vancomycin. The target AUC is 400 to 600 μg∙h/mL5). Trough values were previously used in clinical practice as an alternative to AUC. The correlation between trough values and AUC, however, has been reviewed in a recent study which reported that AUC cannot be accurately estimated based on trough value alone. This study reported that both peak and trough values are needed to accurately estimate AUC6,7). The peak value is an important factor in the calculation of AUC, since the drug half-life is defined by the difference of the peak value from the trough value and distribution volume is defined by the peak value.
The efficacy and safety of vancomycin are evaluated based on AUC, with the target range of 400 to 600 μg∙h/mL. Both peak and trough values are needed to accurately determine AUC. In line with this, software (Practical AUC guided TDM for vancomycin: PAT) was developed to enable dose design based on AUCs. The program requires blood concentrations to be measured on the third dose before steady-state. For twice-daily dosing, the blood concentration measurement is performed on the second day of treatment. As shown in Figure 4, on the following day after blood sampling, blood concentration analysis with the LM1010 high-speed liquid chromatograph will be conducted for patients who are kept on vancomycin based on the results of the Verigene® system. The data are fed into PAT to design a treatment regimen for achieving the target AUC to optimize vancomycin treatment. Unlike the blood culture test, the Verigene® system can reveal antimicrobial resistance the next day following blood sampling (i.e., result obtained quicker than blood culture). If mecA is not detected, vancomycin will be discontinued, which will in turn eliminate the need to monitor blood drug concentrations, thereby reducing the workload.
Table 4 Days of blood concentration analysis for antimicrobials indicated for TDM, target AUC (in μg∙h/mL), and peak/trough values (in μg/mL)

*In combination therapy for gram-positive bacteria, a peak of 3 to 4 μg/mL and trough of < 1 μg/mL should be targeted.
Hepatic injury is the most common adverse reaction caused by the antifungal voriconazole. The incidence of which is listed as 36.0% in the Japanese package insert and 12.2% in the United States. Wild-type CYP2C19 (the primary metabolic enzyme of voriconazole) is found in 30% to 40% of the Japanese population and around 70% of Westerners8). This means that 60% to 70% of the Japanese population has a CYP2C19 mutation. It is postulated that this mutation reduces the ability to metabolize voriconazole, which results in an increase in blood concentrations and a higher incidence of hepatic injury. TDM is therefore recommended for voriconazole, the only antifungal indicated for TDM.
Blood levels were measured on days 3-5 of treatment, with a target trough value of 1-4 μg/mL (Table 4). Voriconazole is administered at a loading dose of 6 mg/kg twice daily on day 1 and at a maintenance dose of 3-4 mg/kg twice daily on days 2 and beyond. We performed a population pharmacokinetic analysis to determine the maintenance dose that would result in a trough concentration of 2-4 μg/mL9). From the results of our study, the recommended doses were 3.6-4.5 mg/kg twice daily for the wild-type CYP2C19 patients and 2.2-3.3 mg/kg once daily for the mutant patients. Therefore, a dose of 4 mg/kg per dose can be safely used for the American patients with predominantly wild-type CYP2C19, but for the Japanese patients with predominantly mutant CYP2C19, a dose of 3 mg/kg per dose is considered to be a guideline for safe use.
However, since early treatment is important in severe infections, the maintenance dose should be 4 mg/kg per dose for the patients with CYP2C19 mutation to avoid treatment failure. In such cases, if genetic polymorphism analysis can be performed with the patient's consent, optimal medical care can be provided to the patient. The DS3000 compact capillary electrophoresis sequencer can complete CYP2C19 gene analysis in about 8 hours. Conducting gene analysis on the first day of voriconazole treatment would allow the proper maintenance dose of either 4 mg/kg for wild-type CYP2C19 or 3 mg/kg for mutant CYP2C19 to be selected on day 2 of treatment (Figure 5). Blood levels are then measured on days 3-5 of dosing. Voriconazole concentration is an outsourced test in most medical institutions, and it takes more than one week from the start of administration to obtain the blood concentration results. Voriconazole can be used safely if genetic polymorphism analysis is performed in advance and the dosing regimen is decided based on the results. In addition, one of the key features of the LM1010 high-speed liquid chromatograph is its ability to determine voriconazole concentrations. Medical institutions that own the LM1010 can perform same-day concentration analyses. So if the patients show signs of deterioration or development of liver injury, the clinician can check the blood levels immediately and decide on the same day to increase or decrease the voriconazole dose or change to another drug, instead of having to wait until 3-5 days for the blood levels, thereby optimizing treatment in a timely manner.
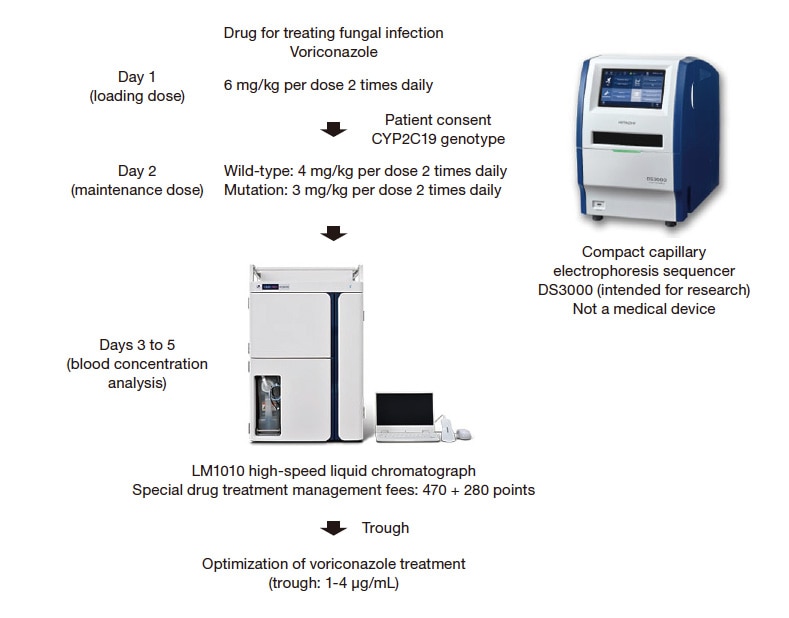
Fig. 5 Treatment optimization based on CYP2C19 genetic polymorphism analysis and blood drug concentration analysis for voriconazole
Linezolid is a drug to treat MRSA and VRE infections when warranted by the detection of the drug-resistance gene mecA or vanA using the Verigene® system. Linezolid is administered at 600 mg twice daily. The main side effect is thrombocytopenia, which occurs very frequently (8-68%)10). We searched for a blood concentration window for linezolid that provides efficacy while minimizing thrombocytopenia and found a correlation between the trough value of linezolid and the incidence of thrombocytopenia, with a 50% incidence of thrombocytopenia occurs at a trough value of 8.2 μg/mL.
Furthermore, population pharmacokinetic analysis revealed that a trough value of at least 3.6 μg/mL was necessary to achieve the linezolid PK/PD target of AUC/MIC ≥ 100 in strains with a MIC ≤ 2 μg/mL10). Considering the reports of other research groups, the effective trough value of linezolid is estimated to be ≥ 3-4 μg/mL and ≤ 6-7 μg/mL. Linezolid is a difficult drug because of its high incidence of adverse reaction, but it is safe and effective when administered guided by this target trough value range. Another key feature of the LM1010 high-speed liquid chromatograph is its ability to determine linezolid concentrations. Linezolid can be therapeutically optimized by determining the trough value of linezolid on day 3 of treatment (with the consent of the patient) and using the result for dosing adjustment to achieve the target trough value.
Rapid genetic testing and measurement of drug blood levels are essential for the practice of AS. The availability of instruments that enable these analyses allows clinicians who can use them to improve patient outcomes, reduce the likelihood of bacterial drug resistance, and lower the cost of medical care.
References
See more
