
Kana Matsumoto
Ph. D.
Associate Professor
Department of Clinical Pharmceutics,
Faculty of Pharmaceutical Sciences,
Doshisha Women’s College of Liberal Arts
This article introduces cases in Japan. (The SI NEWS Editorial Office)
TDM, which stands for therapeutic drug monitoring, is a type of individualized treatment design based on the blood concentrations of the drug being used or its metabolites. TDM was first used in clinical practice in Japan in early 1980s and became established in clinical practice when TDM fees, classified as special drug treatment management fees, subsequently gained insurance coverage. Currently, the number of covered drugs has grown up to about 40. TDM has recently been used for several drugs not eligible for special drug treatment management fee reimbursement. Healthcare professionals are now well aware that TDM facilitates individualized treatment design and evidence-based drug therapy, and helps investigators make new pharmacokinetic findings.
Successful TDM obviously requires proper blood sampling technique and timing, and proper handling of samples. Large variations in the timing of blood sampling and errors in blood sampling technique and sample handling, however, occur in clinical settings. We have seen such errors result in misinterpretation of data that has could have put the lives of patients at risk.
This article discusses errors related to blood sampling technique and sample handling associated with TDM that I have witnessed, describes TDM coursework offered by the college where I teach to eliminate such errors, and presents efforts to bridge between education to clinical practice.
The college laboratory I lead (hereafter referred to as “the Laboratory”) conducts patient pharmacokinetics (PK) studies in partnership with medical institutions nationwide. These studies proceed as shown in steps 1 to 12 in Figure 1. However, there are errors in the blood samples and sheets that contain patient information needed for our analyses that the medical institutions sent, and these errors often make it difficult for us to properly measure blood drug concentrations and conduct proper analyses. For example, sample handling errors and other errors that occurred in a TDM study of the anticancer agent busulfan used as the conditioning regimen for hematopoietic stem cell transplantation are shown in Figure 2. The Laboratory received 626 samples collected from 145 patients at 23 medical institutions nationwide to measure blood busulfan concentrations. We classified the errors that occurred from the time busulfan was administered to shipment receipt of samples at the Laboratory (Figure 1, steps 4 to 9) into 9 categories and then counted the number of errors in each category. The most common errors were seen in the patient and sample information. We were able to resolve input errors and missing data by querying the medical institutions, but we were forced to exclude the data of 18 patients (12.4%) with an incorrect infusion time, incorrect sampling time, or incorrect sample storage from the final analyses. We had to classify the data of these patients as “for reference only” when we sent the results back to the medical institutions.
These samples represent just the tip of the iceberg of the many TDM samples collected day after day across Japan. Seeing many errors associated with the relatively small number of samples we analyzed, we began to wonder just how many treatment design regimens based on TDM data formulated in medical institutions throughout the country were of questionable reliability, and were compelled to feel tremendous anxiety. In the next section, I will discuss the TDM coursework that the college where I teach (hereafter “the College”) offers to help resolve this situation.
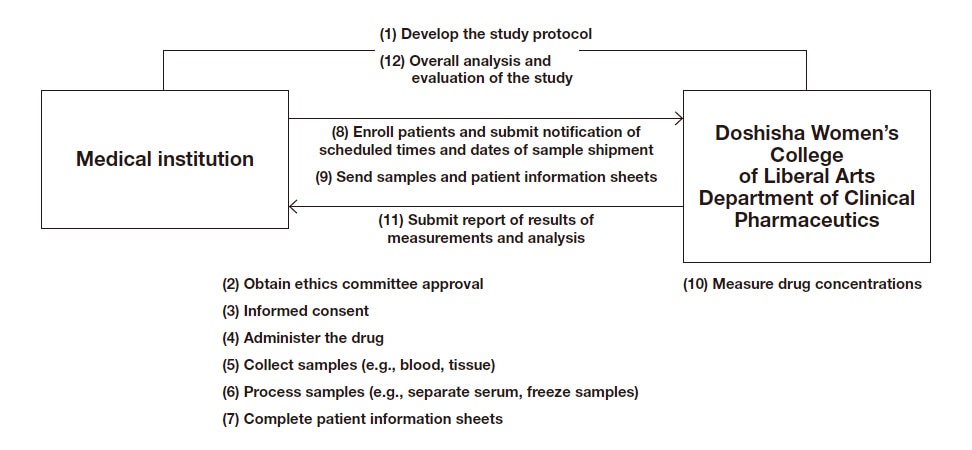
Fig. 1 Flow of a clinical pharmacokinetics study
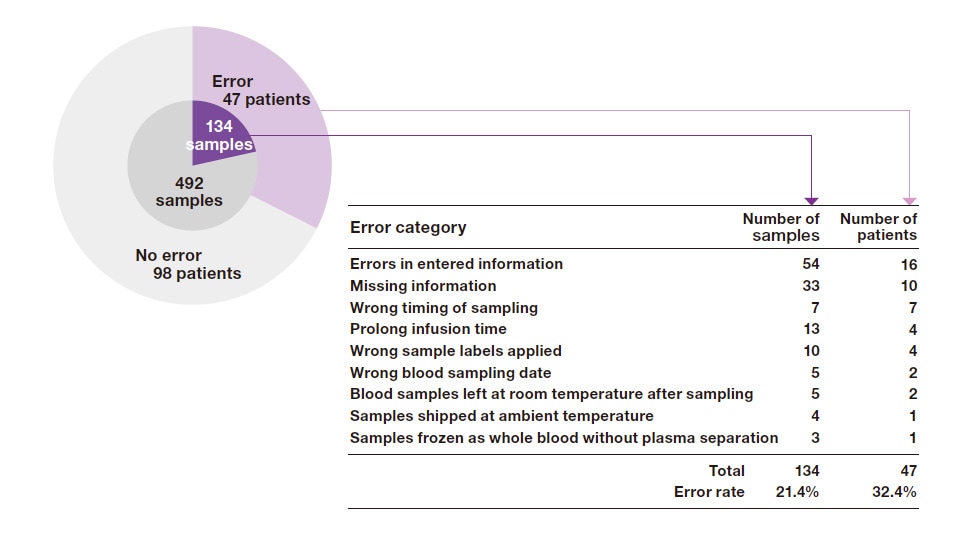
Fig. 2 Sample handling errors and other errors that occurred in a TDM study of busulfan
The College became convinced that university education placed on PK analysis focusing only on analysis after blood drug concentration data are obtained is responsible for the high incidence of sampling errors and sample handling errors associated with TDM discussed in the previous section. In response, we have offered coursework that goes beyond data analysis to help students appreciate the importance of timing of blood sampling to accommodate the condition of the patient and pharmacological characteristics of the drug and of sample handling, since these underpin TDM. Some components of this coursework are presented here.
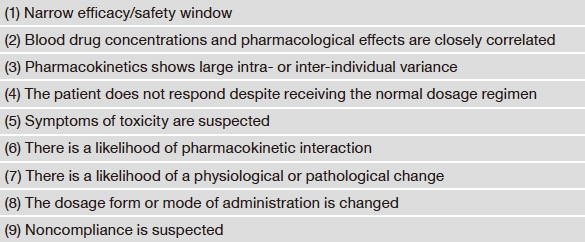
To qualify as a drug for which TDM is needed, a drug must satisfy the first 3 criteria listed in Table 1, namely (1) have a narrow efficacy/safety window, (2) blood drug concentrations and pharmacological effects are unequivocally correlated, and (3) pharmacokinetics shows large intra- or inter-individual variance. These criteria qualify the 40 drugs mentioned earlier for TDM in terms of health insurance coverage. Table 1 also lists situations in which TDM is required for these drugs, namely (4) the patient does not respond despite receiving the normal dosage regimen, (5) drug toxicity is suspected, (6) there is a likelihood of PK interactions, (7) there is a likelihood of a physiological or pathological change, (8) the dosage form or mode of administration is changed, and (9) noncompliance is suspected.
Although TDM represents a tool for increasing the quality of drug therapy in situations 4 to 9, caution is needed because it cannot prevent all adverse reactions and exacerbation. Taking situation 6 (drug interactions) as an example, TDM can only detect PK interactions associated with changes in blood concentrations and not pharmacodynamic interactions with no changes in blood concentrations. Fluoride excess caused by voriconazole1,2) is an example of a toxicity (adverse reaction) difficult to detect and prevent in situation 5. One of the papers on this adverse reaction1) reported a mean plasma concentration of voriconazole of 1.52 μg/mL in the affected patients (target concentration range: 1 to 5 μg/mL), which is certainly not high and unlikely related to adverse reaction onset. We concluded that the long duration of treatment, with a mean of 21 months, rather than blood drug concentrations, was considered to be the risk factor for fluoride excess.
Table 1: Drugs and situations for which TDM is warranted
The efficacy and safety windows normally established for TDM are based on blood concentrations that have reached a steady-state condition. Blood samples for TDM are therefore generally collected and measured after the concentration has reached a steady-state condition. As shown in Figure 3, measured values (see the black circle) determined from blood collected before a steady-state condition is reached mistakenly indicate that the level is too low, leading the clinician to escalate the dose. The drug concentration can reach the toxic range by the time the steady state is reached. The time required for a steady-state condition to be reached varies by drug, but it is typically about 4 to 5 times the halflife of the drug in question.
Waiting for a steady-state condition to be reached in antimicrobial treatment for patients with severe infections, however, can delay the time when the dose is adjusted to a proper level, which can in turn result in the death of a patient that could have been saved. Such situations demand flexibility, such as sampling before the steady state is reached and then analyzing the blood using a program that simulates pharmacokinetics so that the steady-state blood concentration can be rapidly predicted.
Another important consideration is the time from the last dose to blood sampling. TDM is essentially performed to determine whether the drug has reached a concentration in the target tissue necessary for efficacy (or toxicity), which requires equilibrium to have been reached between the blood concentrations being measured and concentrations in the target tissue. Concentrations determined with blood sampled before the two have reached equilibrium are therefore not indicative of efficacy and toxicity in the target tissue. The blood concentration profile associated with oral digoxin use in Figure 4 is a typical example of this situation. For about 6 hours after digoxin treatment is started, the drug is still being absorbed via the gastrointestinal tract into the systemic circulation and from the circulation into the tissues (alpha phase). In this phase, blood concentrations are not yet in equilibrium with tissue concentrations. TDM for digoxin requires blood to be sampled and measured in the beta phase, which begins after equilibrium is reached. If the blood is collected at nonspecific times without taking this requirement into consideration, the concentrations may appear to vary greatly from day to day and lead to misinterpretation.
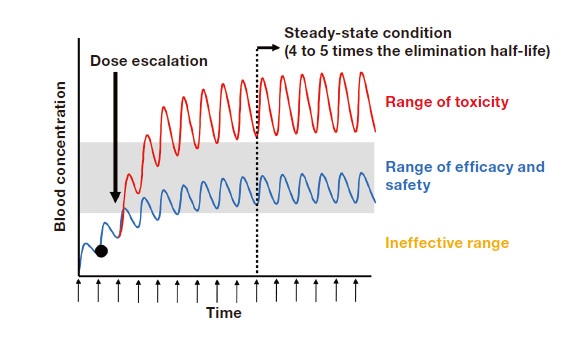
Fig. 3 Example of dose escalation based on measured values determined before a steady-state condition is reached
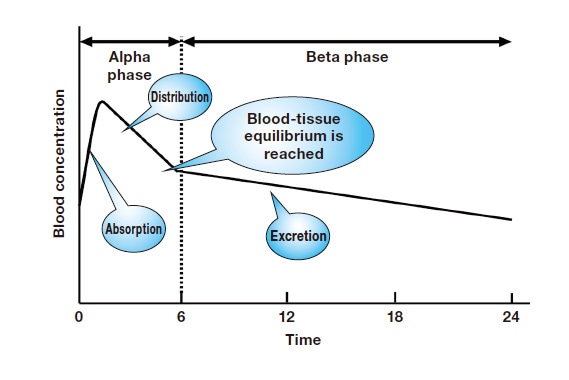
Fig. 4 Blood concentration profile after the start of oral digoxin
The samples used for TDM are typically serum or plasma, and most of the case both yield similar measured values. However, since there are exceptions, the differences in these samples should be clearly understood.
Plasma: Supernatant obtained by centrifuging blood that is sampled in a tube pretreated with an anticoagulant such as EDTA or heparin to precipitate away blood cells.
Serum: Supernatant obtained by centrifuging blood that is collected in a tube not pretreated with an anticoagulant and then allowed to stand for about 30 minutes at room temperature so that the blood cells coagulate.
TDM performed at medical institutions (i.e., that qualifying for special drug treatment management fee reimbursement under insurance) is normally done with serum samples, except in the case of immunosuppressant therapy discussed later. This is because serum is less expensive than plasma to obtain since no anticoagulant is needed, and it does not contain an anticoagulant such as EDTA or heparin that could interfere with the analysis. If the drug in question is a positively charged aminoglycoside antimicrobial agent, it could form a complex with negatively charged heparin that could interfere with the analysis or, if the sampling tube contains a serum separating agent, the drug in question may be adsorbed to that agent, which could make the results inaccurate. When the Laboratory performs TDM of a carbapenem antimicrobial agent such as meropenem3,4) or the anticancer agent melphalan5) in a collaborative study with medical institutions, we find ourselves unable to accurately determine concentrations using serum samples, which must be kept at room temperature for 30 minutes after blood sampling until coagulation is complete, because these drugs break down very rapidly in blood samples, in matter of minutes. In these cases, plasma is the preferred sample type because it can be quickly obtained from sampled whole blood after blood sampling6).
There are also drugs that are best analyzed using whole-blood samples. Typical examples are the immunosuppressants cyclosporine, tacrolimus, and everolimus. When in the blood, a large fraction of these drugs bind to special proteins present in red blood cells, meaning that the portion of these drugs present in red blood cells must be included. Blood is collected in a tube treated with EDTA and then subjected to hemolysis to release the fraction of the drug in the red blood cells so that it can be measured.
Many procedures including immunoassays and high-performance liquid chromatography (HPLC) are used to determine concentrations of drugs in the blood. Whether analyses are performed internally or delegated to a contract laboratory using any procedure, the requirements listed in sections 3-1 to 3-3 above must be properly implemented and verified.
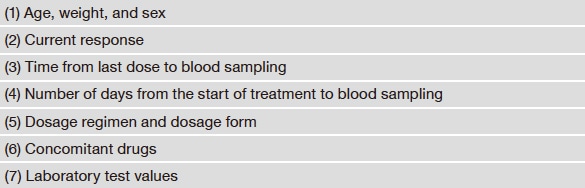
Once blood concentration measurement is complete, the data must be analyzed. Information needed in this stage is shown in Table 2. Undertaking treatment design based on the PK data alone without a full picture of this information can lead to misinterpretation. For example, if the current response (Table 2, item 2) is poor even though the blood concentration is suitably within the target range, confirming whether the time from the last dose to blood sampling (Table 2, item 3) is appropriate is necessary. Obviously, information including the drug administration (dose), blood sampling procedures, sample handling, and analytical procedures must also be fully checked and factored into the results.
Table 2: Patient information relevant to data analysis
We designed the TDM coursework discussed earlier for students of our College. We give students in the Laboratory the opportunity to analyze actual patient samples and experience everything from data analysis to reporting, aiming to provide an immersive experience. Students can gain invaluable experience through involvement in TDM studies where they are required to handle patient samples and information and integrate the results they personally produce into treatment decision-making. When these students graduate and begin working at a medical institution, we are convinced that they will be able to leverage this experience in designing drug treatment regimens optimized for individual patients, even when they do not personally perform blood concentration analysis internally. We are also seeking ways to provide lifelong and postgraduate learning opportunities of handling patient samples and measuring blood concentration using HPLC for pharmacists working in community settings.
It is my sincerest hope that the students who complete the coursework discussed in this article successfully bridge education and clinical practice as the next generation of pharmacists, thereby helping to improve and expand the quality of TDM in Japan.
References
See more
